Integrating domestic animals into palliative care environments reduces measurable physiological distress, yet healthcare systems routinely fail to operationalize this intervention due to fractured regulatory frameworks and unquantified risk vectors. Current legislative efforts, such as the statutory framework introduced to the Polish parliament by lawmaker Katarzyna Piekarska, attempt to codify a universal right for terminally ill patients to receive visits from their own companion animals. This legislative push, accelerated by clinical precedents at the Medical University of Warsaw under Dr. Tomasz Dzierżanowski, highlights a critical systemic bottleneck: the historical reliance on ad-hoc, discretionary permissions rather than standardized clinical protocols. Optimizing end-of-life care requires moving past sentimentality to analyze the precise biological mechanisms, operational friction points, and risk-mitigation strategies inherent in institutional animal visitation.
The Dual-Pathway Mechanism of Human-Animal Interaction
The clinical efficacy of human-animal interaction in a palliative setting operates via two distinct biobehavioral pathways: neuroendocrine modulation and the mitigation of existential isolation. Human clinical trials consistently demonstrate that structured interactions with familiar or therapeutic animals yield immediate changes in a patient's neurochemical profile.
Neuroendocrine Regulation
The presence of a companion animal triggers a down-regulation of the sympathetic nervous system (SNS) and the hypothalamic-pituitary-adrenal (HPA) axis. This shift is characterized by quantifiable biomarkers:
- Cortisol Reduction: Serum and salivary cortisol levels decrease rapidly during tactile interaction with an animal, mitigating the physiological markers of acute stress.
- Oxytocin System Activation: Mutual gaze and physical contact between humans and dogs or cats stimulate the endogenous release of oxytocin, which suppresses amygdala hyperactivity and lowers subjective pain perception.
- Autonomic Stabilization: Patients exhibit an increase in heart rate variability (HRV) and a concurrent reduction in mean arterial pressure, shifting the autonomic balance toward a parasympathetic state.
The Mitigation of Existential Isolation
Dr. Dzierżanowski identifies an "epidemic of loneliness" affecting two distinct cohorts in contemporary palliative wards: geriatric patients who have outlived their primary social networks, and younger patients whose digital networks fail to provide somatic or emotional presence during active dying. Domestic animals function as non-judgmental attachment figures. Unlike human interactions, which can be fraught with complex familial grief and conversational strain, animal interactions require no verbal processing. This reduces the cognitive and emotional load on a failing physiological system.
Operationalizing the Distinction: Patient-Owned vs. Facility-Aided Animals
A major logical failure in existing healthcare administration is treating professional therapy animals and personal pets as interchangeable assets. They occupy entirely different positions within an institutional cost-benefit matrix.
Therapy Animals (The Controlled Variable)
Certified therapy animals, such as the Australian Shepherd utilized at the Warsaw clinic, operate as highly standardized clinical inputs. They undergo rigorous behavioral screening, possess predictable temperaments, and follow strict veterinary sanitation schedules. Their presence serves as a generalized distraction and acute stress reducer for both patients and healthcare staff, including nursing and culinary personnel. The primary limitation is the lack of a specific biographical bond; the intervention is therapeutic but not deeply personal.
Patient-Owned Pets (The Biographically Bound Asset)
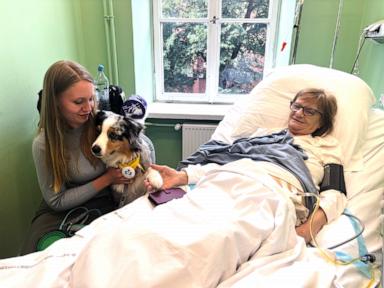
The introduction of a patient’s own pet—such as the cats that inspired the Polish legislative push, or the shelter dog Gaja belonging to patient Ewa Lutka-Krawczyk—addresses deep-seated separation anxiety. The mechanism here is bidirectional. When a terminally ill patient is institutionalized, the animal at home frequently exhibits behavioral regression, such as anorexia or separation-induced distress. The patient's awareness of the animal’s suffering creates a psychological distress loop that exacerbates physical pain and spiritual suffering.
Reunification disrupts this loop. The animal's behavioral cues change upon re-establishing physical contact, which provides the patient with explicit confirmation of the animal’s well-being. This removes a major barrier to emotional closure during the final stages of life.
The Institutional Risk Matrix and Mitigating Protocols
Implementing a universal right to pet visitation introduces specific operational liabilities that hospital administrators must manage through structured protocols rather than blanket prohibitions. The risk matrix breaks down into three core vectors.
1. Zoonotic and Epidemiological Control
The introduction of any biological agent into a clinical environment presents an infection risk, particularly to immunocompromised oncological patients.
- The Mitigation Protocol: Passports or veterinary validation logs must accompany any visiting animal, verifying up-to-date vaccinations, external parasite treatments, and a clean bill of health within a 72-hour window prior to admission. The animal must be clean, and wiping paws with antiseptic, pet-safe solutions prior to ward entry must be mandatory.
2. Behavioral Unpredictability and Physical Safety
Medical environments feature high sensory stimulation: alarms, strange odors, unfamiliar personnel, and complex medical apparatuses like draining tubes, intravenous lines, and monitors. This environment can induce a fear-aggression response in a stressed animal.
- The Mitigation Protocol: Institutional frameworks must require animals to remain leashed, harnessed, or contained within specialized carriers during transit through common areas. The visit must occur in a private room or a designated neutral zone. Furthermore, an explicit liability waiver must be signed by the patient's legal proxy or family member, designating a specific handler who remains entirely responsible for the animal’s behavior and immediate removal if stress signals manifest.
3. Environmental and Structural Interference
Wards are shared spaces. Introducing animals poses a direct challenge to patients suffering from severe pet allergies or cynophobia/ailurophobia, and can compromise the sterile boundaries of neighboring clinical zones.
- The Mitigation Protocol: Facilities must implement spatial zoning. Animal visitation should be restricted to designated rooms or wings equipped with independent air filtration systems (HEPA filters) to prevent allergen drift.
Systemic Resource and Economic Cascades
While the primary justification for animal visitation is humanistic, the operational reality within a hospital or hospice system relies on economic and resource efficiency metrics.
[Patient-Pet Separation] ──> [Increased Cortisol & Pain Perception] ──> [Higher Analgesic Demand]
│
[Reunification Protocol] ──> [Neuroendocrine Stabilization] ──> [Decreased Resource Drain]
The standard palliative care model incurs substantial costs through pharmacological management of breakthrough pain and existential agitation. When human-animal interaction successfully lowers a patient's subjective pain scale and stabilizes autonomic markers, the frequency of PRN (as-needed) administrations of high-cost analgesics and anxiolytics decreases.
Furthermore, the secondary benefits extend directly to clinical staff. Palliative healthcare workers experience high rates of secondary traumatic stress and burnout. Interacting with visiting animals or witnessing the psychological relief of a dying patient serves as a low-cost, organic mechanism for staff decompression. This micro-intervention lowers occupational stress indicators and mitigates costly turnover rates among nursing personnel.
The legislative strategy currently advancing through Poland's health committee represents a vital shift from discretionary charity to structural compliance. To succeed, the final statutory language must avoid vague proclamations of rights and instead define the exact veterinary, legal, and spatial parameters required for safe execution. Hospital systems that proactively construct these regulatory frameworks will optimize their resource allocation, lower their pharmacological overhead, and significantly elevate the baseline quality of end-of-life care.



